 Here we go on a reiteration of the glorious wedding between nanotechnology and neuroscience
Here we go on a reiteration of the glorious wedding between nanotechnology and neuroscience:
I did my masters in nanotechnology and every once in a while I go on the net to see what is current out there I am pleasantly surprised. I was happy to run into an article that sits at the intersection of nanotechnology and neuroscience.
Well, maybe I should backtrack and explain what nanotechnology is all about... Fortunately, I do not have to recite in detail all of the copious amount of information that is available on the net about nanotechnology, but the
following article in The New Atlantis gives a very good account of what nanotechnology is all about.. (In a sentence, the human hair is about 80000 nanometers thick - we are talking about devices of the range of 10-20 nanometers thick whereas a red blood cell is vast in comparison: about 5,000 nm in diameter). At this ‘nanoscopic’ level, most of our body cells start to look like giant hot air balloons and a lot of work can be accomplished if we load the right scientific instruments at the end of nanometer sized problems that can then be inserted into our cells.
OK, this is precisely what is happening:
As you know, our brain is richly impregnated by millions of blood vessels whose diameter range from 5 millimeters (the larger junctions) to 10 microns (at the smallest levels). In fact we have about 25 kilometers of blood vessels that have a diameter of less than 10 microns.
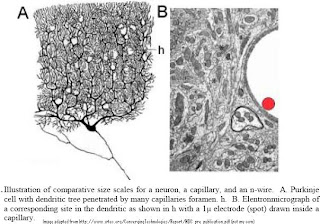
" The basic idea consists of a set of nano-wires tethered to electronics in the main catheter such that they will spread out in a “bouquet” arrangement into a particular portion of the brain’s vascular system. Such arrangement could support a very large number of probes (in the millions). Each n-wire would be used to record, very securely, electrical activity of a single or small group of neurons without invading the brain parenchyma. Obviously, the advantage of such system is that it would not interfere with either the blood flow exchange of gases or produce any type of disruption of brain activity, due to the tiny space occupied in the vascular bed.
A catheter is introduced into the femoral carotid or the sub-clavial artery and is pushed up to one of the vascular territories to be addressed. Such procedure is, in principle, similar to interventional neuro-radiology techniques where catheters are guided to any portion of the central nervous system. The number of 0.5 micron diameter wires (recording points) that could be introduced in a one-millimeter catheter is staggeringly large (in the range of few million). Once the areas to be recorded or stimulated are reached, a set of leads held inside the catheter head would be allowed to be extended and randomly distributed into the brain’s circulatory system. Since a catheter can be placed in any major brain vessels, the maximum length of nano-wire electrodes required to reach any capillary bed is of the order 2 to 3 cm. Hence, a large number of electrodes would cover any region of the central nervous system from the parent vessels harboring the stem catheters. "
This means that most of the brain can be 'reached' using this technique and signals from the 'signal ensemble in our brains' can be dynamically read to yield information on malfunctions, malformations or aberrations. This is extremely exciting and shows yet another way in which new technologies are helping us reach and probe into the deepest parts of the brain without interfering with too much of the inherent functions.
I see a future whereby patients can go a suitably equipped clinic, get this nano wire inserted into her/his femoral carotid and let the vascular system do its work of pulling the wire through all of the arteries that interlace our brains. Once the blood 'pulls' the fibers into the deepest parts of the brain, non-integrated dynamic signals from various parts of the brain can then be mixed and integrated to yield useful information helping us pinpoint tumors, clots, infarcts or damaged brain cells at a microscopic level. A neuro-surgeon can then use the same nano wire apparatus only this time turning on the ablative laser at the end of the nano-wire, find the cells that constitute the tumor/glioma and proceed to vaporize it. At the end of the procedure the nanowires are extracted out of the patients femoral carotid and the patient walks back home. No skull splitting brain surgery or no post operative recuperation... Of course this is me dreaming in the New Year...
That said, I would also urge you to refer to the following words of caution:
“Release of nano-particles should be restricted due to the potential effects on environment and human health.” – Nanotechnology and Regulation within the framework of the Precautionary Principle. Final Report for ITRE Committee of the European Parliament, February 2004.
“Until more is known about their environmental impact we are keen that the release of nanoparticles and nanotubes in the environment is avoided as far as possible. Specifically we recommend as a precautionary measure that factories and research laboratories treat manufactured nanoparticles and nanotubes as if they were hazardous waster streams and that the use of free nanoparticles in environmental applications such as remediation of groundwater by prohibited.” – Royal Society and Royal Academy of Engineering, “Nanoscience and Nanotechnologies: Opportunities and uncertainties,” July 2004.
Some papers of interest:


 Painting Post:
Painting Post:






